Last Updated on 2 hours by Publishing Team
COVID-19 Update
Monday 23rd May
| Transmission Update:
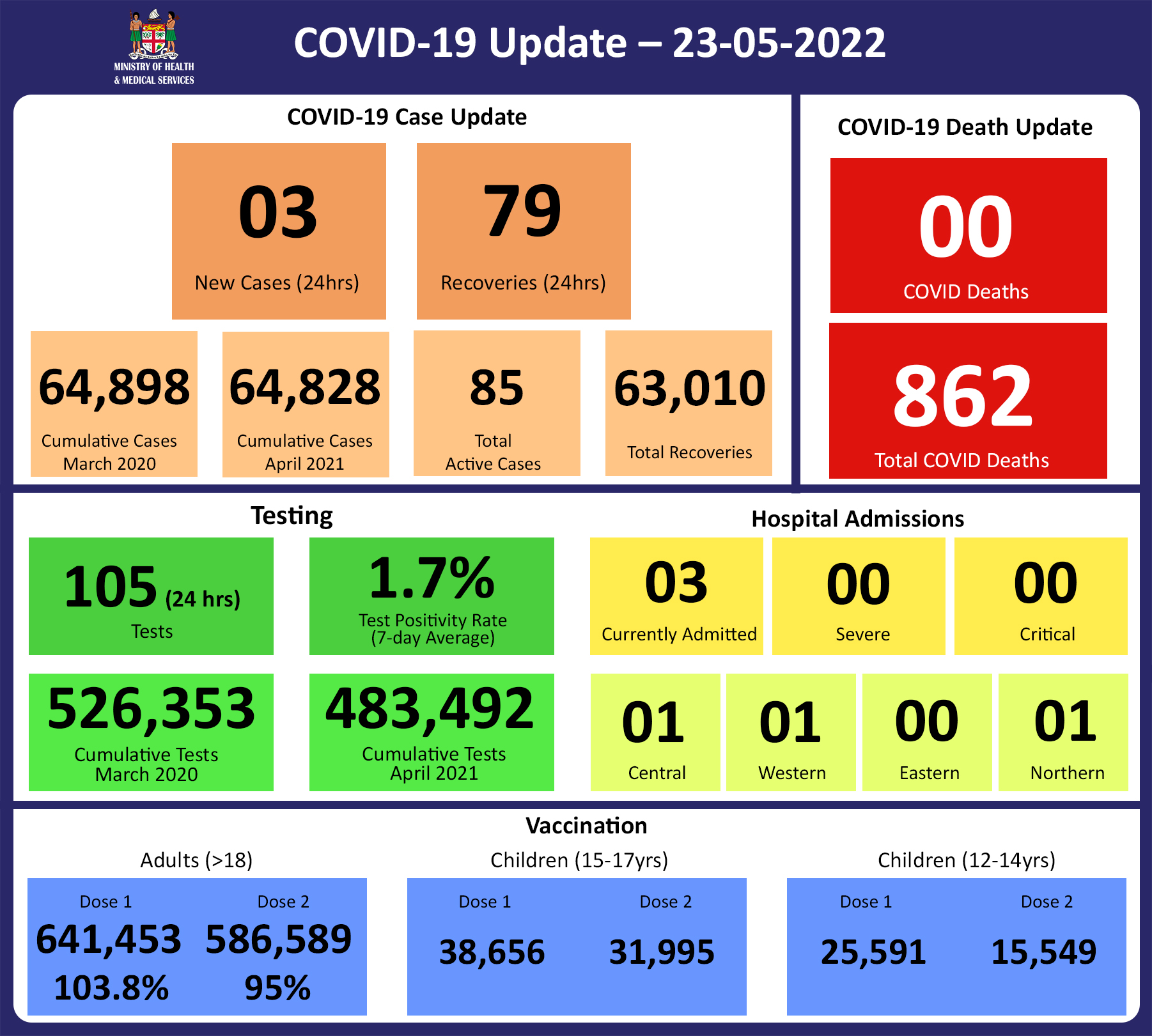
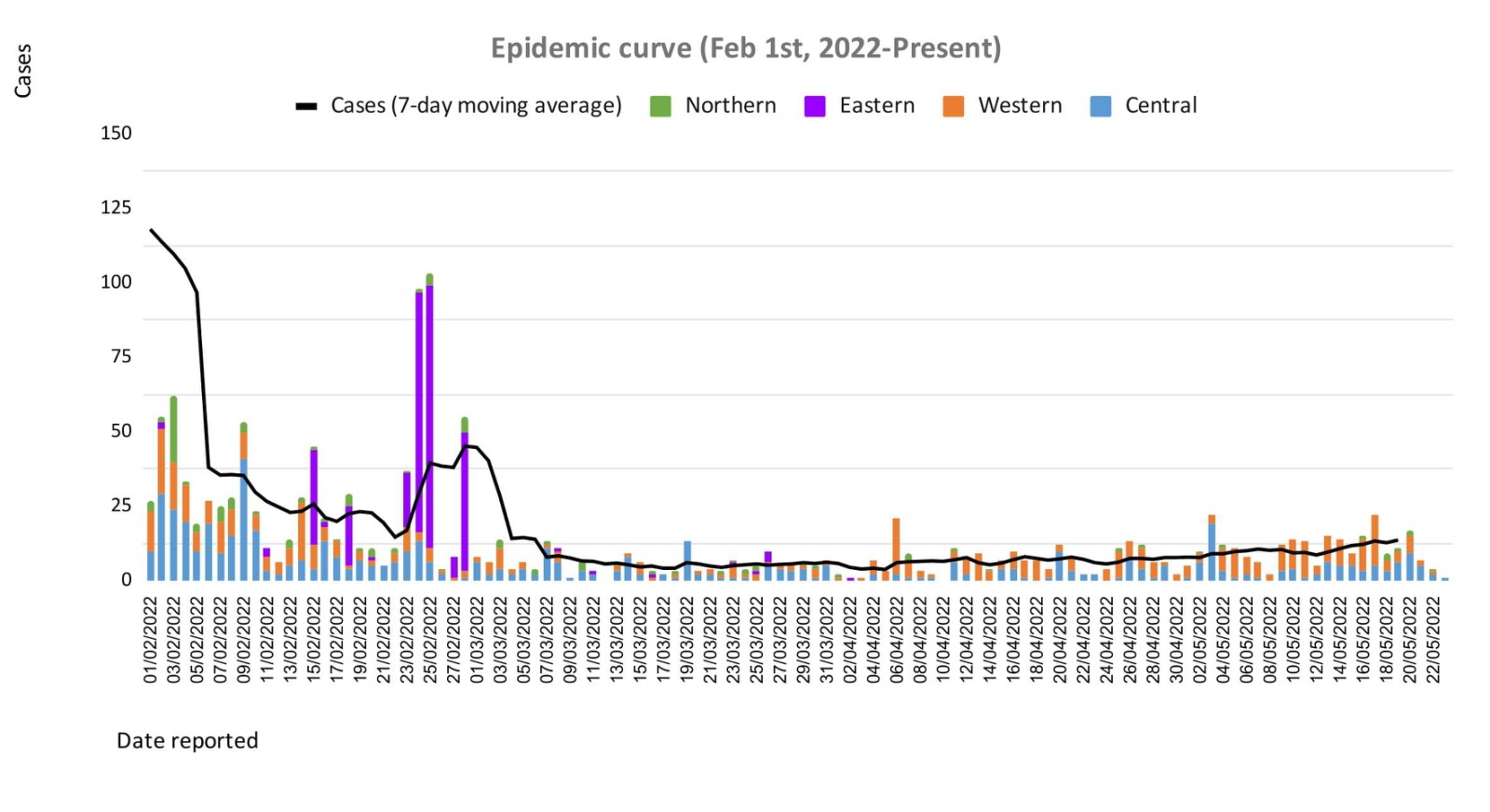
Of the 57 cases recorded, 20 cases were recorded in the Central Division; 33 cases were recorded in the Western Division; 4 cases were recorded in the Northern and nil cases were recorded in the Eastern Division. The national 7-day rolling average of cases as of 19th May is 14 daily cases. The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Deaths:
Analysis of Deaths in the Third Wave Table 1: Death rates by Division
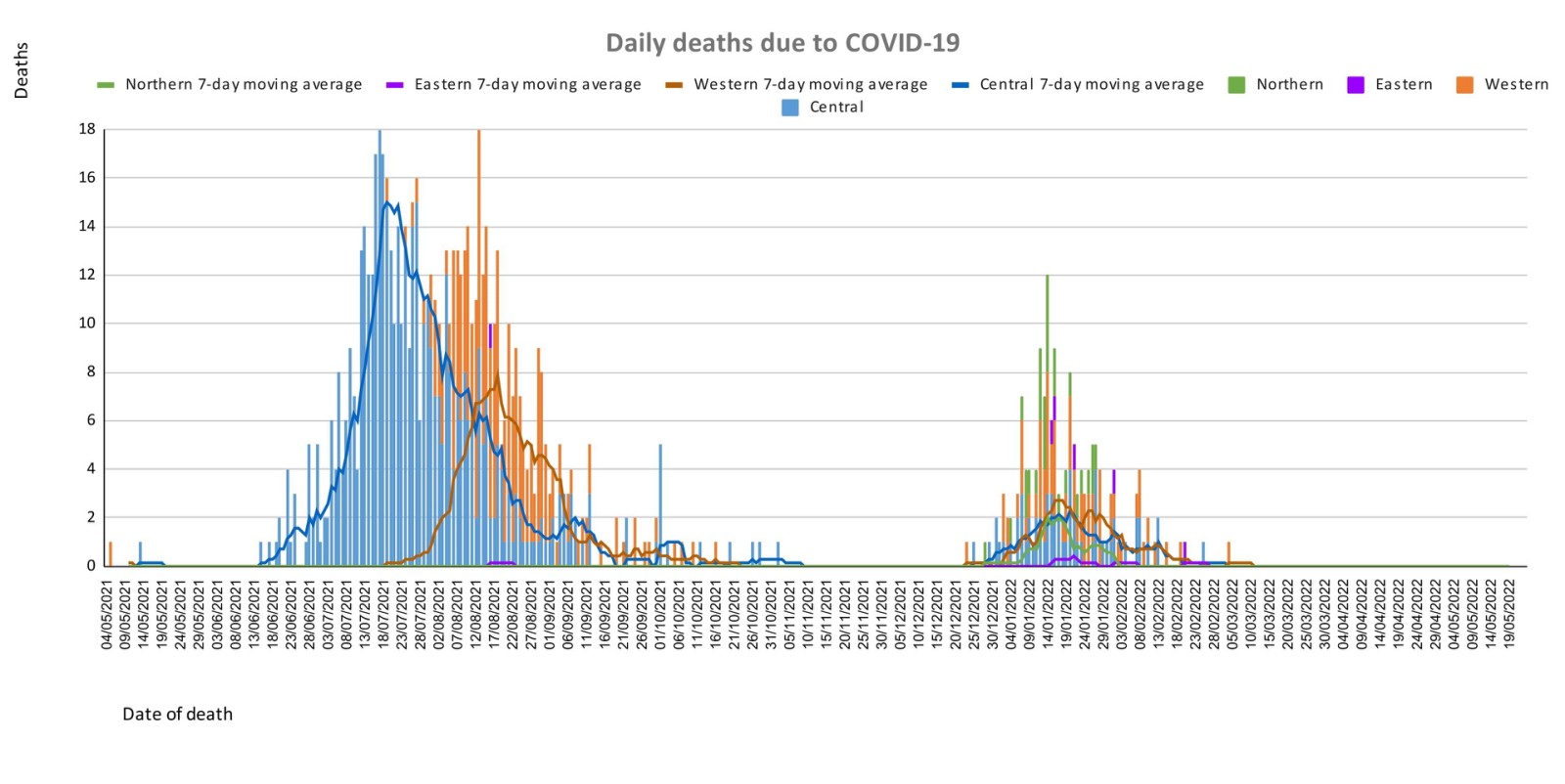
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population. Table 2: Deaths by Age Group
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition. Table 3: Deaths by Vaccination Status
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine. There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported. We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, there are 67% (n=2) cases in the asymptomatic and mild category, 33% (n=1) are categorized as severe and nil cases in the moderate and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testing:
105 tests have been reported for May 22nd, 2022. Total cumulative tests since 2020 are 526,353 tests. The 7-day daily test average is 827 tests per day or 0.9 tests per 1,000 population. The national 7-day average daily test positivity is 1.7%, which is within the WHO recommendation of 5%. |
Public Advisory
COVID-19 trends
We have noted an increasing trend in cases. While the increase is not obvious on our epidemiological curve graph we are maintaining close surveillance of case numbers. We are monitoring hospital admissions and testing for COVID-19. As indicated above while our admissions for COVID-19 remain low, this is an indicator that remains important to our ongoing response plans. The case trends do highlight the need to escalate our booster dose coverage.
International communicable disease outbreaks
AS previously mentioned, the Ministry’s Fiji Centre for Disease Control (Fiji CDC) and Border Health Protection Unit (BHPU) are monitoring international outbreaks of concern, which include Ebola Virus Disease in the Democratic Republic of Congo, Japanese Encephalitis in Australia, acute hepatitis of unknown origin in multiple countries, and monkeypox in the United Kingdom and other countries. Where appropriate, specific interventions have been put in place or strengthened in response. The situation will continue to be monitored, assessed, and responded to based on the available scientific evidence, best practice, and advice from expert authorities.
Monkeypox
As we continue our recovery path during this pandemic, the strategies for resilience require urgent and early preparedness and response planning against any potential threat.
Monkeypox is a rare disease that is caused by infection with the monkeypox virus. It is endemic to certain countries in Central and Western Africa, and the causative virus is of the same family as the smallpox virus. Monkeypox outbreaks have been recently reported in a growing number of countries that are not endemic for the disease, including the United Kingdom, Spain, Portugal, France, Italy, Germany, Sweden, the Netherlands Canada, the United States of America, and Australia.
Monkeypox is usually a self-limiting illness, which means that most people recover with just supportive treatment within several weeks. However, severe illness can occur in some individuals. It does not spread easily between people but person to person transmission may occur through:
- contact with clothing or linens (such as bedding or towels) used by an infected person
- direct contact with monkeypox skin lesions or scabs
- exposure to respiratory droplets eg through coughing or sneezing
The Ministry is working with communications and community engagement teams on appropriate public advisories. We need to arm ourselves with the knowledge to protect ourselves to reduce the chances of spread in our community. Infection prevention protocols are currently being put together at the border and in community facilities. One key focus will be to ensure we have the ability to maintain oversight over travellers from selected countries to ensure early diagnosis, treatment, and contact tracing.
Overall symptoms of the virus can include:
- fever, chills, muscle aches, backache, swollen lymph nodes, and exhaustion
- an unusual rash, which typically starts on the face, then may spread elsewhere on the body.
All doctors and Nurses in the community need to ensure they are well informed of how cases present and be vigilant in helping to ensure cases are diagnosed early.
Prevention of transmission of infection by respiratory and contact routes is required. Appropriate respiratory isolation is essential for suspected and confirmed cases. Scabs are also infectious and care must be taken to avoid infection by handling bedding, clothing, and so on. Workplaces especially in key sectors will be asked to escalate their Infection Prevention and Control and ensure practices are maintained.
The major priority for the Ministry of Health and Medical Services is to have a response plan that will include surveillance with rapid response and containment protocols and at the same time have a minimal social and economic impact. A key focus will be on ensuring that those suspected or confirmed to have monkeypox must be able to be managed in a dignified manner with no threat of stigmatization. Each citizen’s duty to contribute to protecting Fiji must be the priority.
We are in discussions with our reference laboratory in Melbourne to ensure access to definitive tests. Our ongoing efforts to have genomic sequencing capability in the Fiji CDC will provide us with greater capacity to deal with infection threats now and in the future.
We are also in discussions with WHO to ensure we preposition access to vaccines and medications used to treat monkeypox.
It is important however to ensure that in escalating community-wide infection prevention and control measures we are responding to current threats and creating communitywide resilience to upcoming threats. Our ongoing engagement in a healthy lifestyle to mitigate NCDs is also part of the overall focus on building back better and stronger.
The Ministry of Health and Medical Services will be disseminating more specific advisories over the next few days to weeks. Further updated knowledge about the monkeypox virus will be shared as they are known.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is better positioned to focus more on health facilities and health care provision capabilities to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision-making and action within the Ministry.
COVID-19 Vaccination
As of the 23rd of May, a total of 127,951 individuals have so far received booster doses. This represents 29.5% of those eligible for a booster dose. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH. We have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 95% adult coverage rate, 90.6% of all persons over 12 years have had 2 doses of the COVID-19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccines, we are now covering the Primary doses for those yet to be vaccinated and for Dose 2 if individuals were vaccinated with either Moderna or Astra Zeneca while the 12-14-year-olds continue with the Pfizer vaccine. The new supplies of MODERNA are expected to be available in-country at the end of the month.
Cold and flu
The Ministry of Health and Medical Services has noted an increase in people becoming ill with cold and flu-like illnesses as we are coming into our dry and cold season. This increase is especially seen in infants and children under the age of 5. The paediatrics department at CWM Hospital is also seeing an increase in children under the age of 5, especially infants, being admitted with acute respiratory illnesses while testing negative for COVID-19 and influenza. It has been expected that as restrictions intended to prevent transmission of COVID-19 were lifted (including mandatory masking, physical distancing, and school and border closures) other respiratory viruses that normally circulate would begin to re-emerge similar to pre-COVID levels, and possibly even at higher levels due to a decrease in population immunity to seasonal viruses, as cold/flu cases were low during the last two years.